
Special Article: Research Article
Austin J Neurol Disord Epilepsy. 2024; 10(1): 1053.
IQ Affection on Theory of Mind Abilities in Individuals with Autism Spectrum Disorder and Down Syndrome
Nazila Shojaeian*
1Department of Clinical and Health Psychology, Universitat Autònoma de Barcelona, Spain.
*Corresponding author: Nazila ShojaeianDepartment of Clinical and Health Psychology, Universitat Autònoma de Barcelona, Spain. Email: nazila.shojaeian@gmail.com
Received: May 07, 2024 Accepted: May 31, 2024 Published: June 07, 2024
Abstract
Objectives: The present study reports the results of Raven’s Progressive Matrices (RPMs) and Theory of Mind (ToM) first-order tasks for individuals with Autism Spectrum Disorder (ASD) and with Down Syndrome (DS) and for typical children. However, there are few studies that have looked at the intelligence of these groups of individuals. Our aim was to investigate the absolute and relative underestimates of Theory of Mind in participants with ASD and DS in relation to Intelligence Quotient (IQ) in two countries. METHODS: A total of 74 Iranian children whose native language was Farsi participated: 24 ASD, 24 DS, and 26 controls. Similarly, 66 Swedish children whose mother tongue was Farsi: 26 ASD, 18 DS and 22 controls aged 6 to 12 years. Matching by age, gender, and socioeconomic status was performed.
Results: Children with higher verbal IQ had absolutely better performance on: Representative Change_ Question, Smarties False Confidence, Sally and Anne False Confidence,
Keywords: Theory of Mind; Autism Spectrum Disorder; Down syndrome; Intelligence Quotient
Introduction
Cognitive abilities are the understanding of mental states about feelings, thoughts, or beliefs in others, referred to as Theory of Mind (ToM). Children with Autism Spectrum Disorders (ASD) with impairments in their own social communication and behavior are known as the most common neurodevelopmental disorder [1]. Children with DS, categorized with a congenital chromosomal disorder, have lower IQ potential than average, gradually declining throughout childhood IQ [2].
Several studies specifically document the IQ average in adults with DS, which ranges from 25 to 70 [3] and consider other broad research or ranges from 35 to 70 [6]. Autistic individuals are thought to have the ability to measure intellectual performance across the developmental period. While IQ is primarily unstable in childhood, all levels of IQ can occur in ASD [4,5]. To address the impairment of ToM understanding in intelligence impairment, one usually relies on studies of children with comorbidity of low IQ or psychiatric disorders such as autism or psychosis [7].
A number of studies have also demonstrated that the ASD group with higher verbal IQ scores and with higher verbal mental age can pass initial ToM tasks at their age [8]. In the study, parents and teachers of children with autism completed the Sensory Processing Measure, (GARS -2), the nonverbal Raven’s Colored task, etc. to clarify the impairment of some features such as nonverbal IQ, sensory processing and social participation that their children show at home and in the classroom [9].
To bridge to previous studies, it is worth noting that the factors verbal memory and performance IQ were documented as the best predictors of social cognitive skills in a study of three groups of children with autism disorders, a profound developmental disorder not otherwise specified, and non-autistic psychiatric disorders who were participants in the “Utrecht Department of Child Psychiatry” [10].
The Wechsler tests IQ contain some tasks to assess verbal intelligence (vocabulary and text comprehension) and performance intelligence (logical thinking and completing pictures). The verbal task of the Wechsler test is often used to assess children with autism. However, results show that comprehension difficulties in this group may reflect their weak abilities regardless of ToM performance [11]. Given the limited narrative language skills in the majority of children with autism and children with intellectual disabilities, it may be appropriate to use the non-verbal intelligence task. Nevertheless, further research is needed to better understand and know how nonverbal IQ influences the development of ToM.
While the relevance between ToM tasks and IQ in different groups of children and adults has been investigated in previous studies and received sufficient attention, foundations of the relevance between IQ and cognitive functions are needed for further research. The aim of the current study was to make a preliminary assessment of ToM performance in children with ASD and DS compared to a typical comparison group matched for age, gender and IQ. In this study, children with ASD and DS were compared to typical adults on first-order measures of ToM performance and IQ.
Tasks, Measures and Scoring
Method participants: A total of 74 Iranian preschool children participated in this study: 24 children with a formal diagnosis of ASD, 24 children with a diagnosis of DS and 26 typical children. The Swedish preschool children were similar: ASD: 26 children, DS: 18. And 22: TD participated. All these three groups matched as closely as possible in socio-economic status, gender and age. The participants were native speakers of Farsi and Swedish and all born in their country and spoke the local language. The children, aged 6 to 12 years, were tested with extended ToM tests and one test was used to assess IQ. Some children belonging to the ASD and DS groups received special education, and only a small number of these groups lived in homes in both countries. The criteria for inclusion in the study included a formal diagnosis of ASD by a psychologist or psychiatrist who is an expert in the field, a clinical diagnosis of ASD by a clinician according to the criteria of the Diagnostic and Statistical Manual for Mental Disorders (DSM-5), and a language level sufficient to answer the questions on the test. In addition, for both Down syndrome (genetic diagnosis of Down syndrome) and TD: IQ > 70 and not diagnosed with a developmental or sensory impairment, the clinical records were reviewed, excluding the requirement for hearing impairment and the diagnosis of comorbid conditions.
Procedure
All tasks and procedures were structured identically in the Swedish and Iranian cultures. A single rest session, lasting 45 to 60 minutes, depends on the children’s diagnoses and conditions in each country.
Instruments
The Raven’s Progressive Matrices (RPMs): The Raven’s Progressive Matrices (RPMs) are a well-validated group of non-verbal tests for assessing intelligence and cognitive abilities in children and adults. It was originally developed by John C. Raven [12], whose primary goal is to study how genetic and environmental aspects influence intelligence. This test has specific items that can be tested in a group or individually. It asks for the missing item to complete a larger pattern and the correct missing item must be selected from a range of response options; it can be used at all ages. Three published versions are currently used for different groups, including 1) Standard Progressive Matrices (SPM) (for the whole age range or abilities, suitable for ages 8 to 65 years), 2) Colored Progressive Matrices (CPM) (for children aged 5 to 11 years, older people and mentally and physically impaired people and non-English speakers) and 3) Advanced Progressive Matrices (APM) (for adults with higher intelligence, such as people aged 11 years to adults). In our study, we used the same version of CPM in Iran and Sweden for the TD group under 12 years of age and for all children with specific disabilities (DS and ASD). For the typically developed children aged 12, the SPM version was used.
In each task, an answer is scored 1 as correct and 0 for an incorrect answer. Thus, there are six choices (response alternatives) in the CPM with 36 matrices evenly divided into three groups of 12 (A, AB, B) (total raw scores ranged from 0 to 36) [13, 14].The CPM consists of 60 items divided into five groups (A, B, C, D & E) of 12 items each (60 items in 5 groups of 12, and the total raw scores ranged from 0 to 60). It is important to note, however, that we used identical versions in both countries to determine children’s IQ and mental age using Raven’s progressive matrices [15]. British norms were used to assess mental age in Sweden, as there is no standardized Swedish version [16]. To standardize the Raven test in Iranian individuals, previous studies have been documented [17].
Sally and Anne task: A classic Sally and Anne task was used to assess the first order of ToM developed by Wimmer and Perner (1983) [18]. To assess children›s understanding of this task, two characters are introduced at the beginning: Sally (who has a basket) and Anne (who has a box). Sally puts her marble in a basket and then walks away. Anne then takes the marble out of the basket and puts it under the box. While Teddy Sally returned, the experimenter asked: Where does the doll girl Maryam think her marble is? (Belief question). If the children pointed to the previous place (the basket), they admitted a false belief and could pass the question. After that, «Where is the marble?» (Reality question) and «Where was the marble in the beginning?» (Memory question) were asked. The children must achieve total ToM scores between 0 and 3 [19].
Smarties tube task: A child has a tube of Smarties in front of him, which contains a pen instead of the expected Smarties, and asks two controls: “What do you think is in here? The experimenter shows the children the contents and closes the box again, then asks: When the next child comes in, what will he think is in here, does it exist if the child predicts what other people will think (Smarties or chocolate) and What was really in the box? (Pencil) [20].The total score is 0 (fail) or 1 (pass) [21].
Representational Change Test (Picture Task): This task was developed by Gopnik and Astington [22], who first presented a picture of animals whose bodies were covered except for one part (the objects resembled the versions the children had already seen, except for the last picture). Then the investigator showed the child the last picture and asked three questions: What does the child think the object is at the beginning? (Change in representation), if another child comes in (who has not seen the last object), what will he think the object is (false belief)? Also, what does the object look like and what does it really look like (distinction between appearance and reality). The total score ranges from 0 to 3 [22]. We have not found any study on the reliability and validity of the Representational Change Test.
Data Analysis
For data analysis, we used the SPSS 25 program (IBM Corp, 2013) to analyses our results. The results of the experimental measures were analyzed using the method ANOVA. The association between variables was assessed using a one-way ANOVA and a correlation coefficient. A descriptive analysis of the socio-demographic outcomes and the variables in the sample was performed, using the mean and standard deviation for the quantitative variables and the frequency and percentage for the categorical variables. Analysis of variance was used to assess differences between groups on the ToM tasks.
Results
The primary prediction was that children with a higher intelligence quotient would perform better on ToM tasks, regardless of the group to which they belonged. The data analyses for the IQ relationship to the current four subscales on all orders of Theory of Mind are presented in Table 1.
![]()
Mean (
), and (SD)
T/F
Sig.
95% confidence interval
Lower Limit
Upper Limit
Smart_FT
No answer
72.05 (21.110)
-3.348
< .001
Answer
85.16 (23.504)
Smart_N
No Answer
66.73 (15.499)
-2.915
0.004
Answer
82.17 (23.854)
Smart_RQ*
No Answer
73.79 (19.750)
-1.876
0.063
Answer
82.03 (24.373)
S_A_C_FT
No Answer
71.46 (21.179)
-4.194
< .001
Answer
87.46 (22.888)
S_A_M
No Answer
64.77 (19.788)
-5.631
< .001
Answer
86.76 (21.688)
S_A_R*
No Answer
77.03 (24.727)
-0.723
0.471
Answer
80.50 (23.067)
Repr_Q
No Answer
68.06 (21.528)
-4.558
< .001
Answer
85.90 (21.887)
Repr_RD
No Answer
70.11 (18.554)
-2.977
0.003
Answer
83.12 (24.001)
Repr_FB*
No Answer
76.31 (23.291)
-2.324
0.022
Answer
86.04 (22.206)
Note: Mean (x ¯), Standard Deviation (SD), T-test for equality of means (T), significate (Sig.) SAC (Sally and Anne test; FB: False Belief, M: Memory, R: Reality), Smart (smarties tube task;FT: false belief, N: Naming, RQ: reality question), Repr_BF (representational change task, false belief), Repr_Q (representational change task, Question),Repr_RD ( representational change task, Reality Distinction)
Table 1: Statistical Analyses of Correct and Incorrect Answers on ToM Tasks in Terms of IQ (Iran and Sweden).
The results of this study are consistent with previous work suggesting that children with ASD show skill development with higher IQ scores. Thus, we found clear significant correlations between the nonverbal IQ and the first order false belief subscales: Smart_ FT (T = -3.348, p <.001), S_A_C_ FT (T = -2.915, p <.001), S_A_M (T= -5.631, p <.001), Repr_Q (T= -4.558, p <.001). For the remaining tasks: Smarties - Reality Question and Naming, Sally and Anne - Reality, and Representation Change - False Belief and Reality, no differences were found in either country. Therefore, the current results suggest the possibility of passing the False Belief ToM task by accurately predicting higher IQ levels in both DS and ASD groups. The multiple column shows the IQ means of the false and correct responses of all variable tasks. Figure 1.
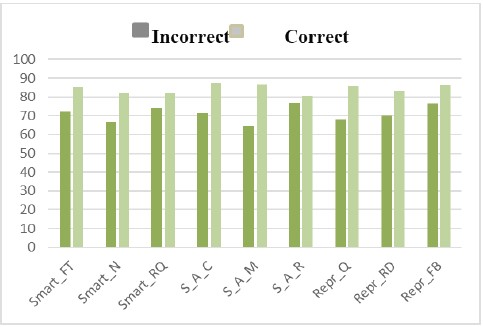
Figure 1: IQ Means the Incorrect and Correct Answer in Each Tasks of ToM.
The mean score of IQ in Iranian children with ASD: 74.30, DS: 70.13 and TD: 103.15 was presented in Table 2. On the other hand, Swedish children with ASD: 76.73, DS: 48.53 and TD: 94.09 scored in their mean IQ. See Table 2.
![]()
IQ
Group (N)
Mean (
), and (SD)
Desv. Error
95% confidence interval
Lower Limit
Upper Limit
Iran
ASD (23)
74.30 (21.455)
4.474
65.03
83.58
DS (24)
70.13 (8.941)
1.825
66.35
73.9
TD (26)
103.15 (14.136)
2.772
97.44
108.86
Sweden
ASD (26)
76.73 (23.535)
4.616
67.22
86.24
DS (17)
48.53 (13.201)
3.202
41.74
55.32
TD (22)
94.09 (10.075)
2.148
89.62
98.56
Note: Intelligence Quotient (IQ), Mean (x ¯), Standard Deviation (SD).
Table 2: Means and Standard Deviations in Diagnostic Groups (Iran and Sweden).
The variable RPMs explained high percentages in each condition that were statistically significant in both countries. In addition, a one-way ANOVA was conducted for all variables. The correlation analysis also showed a significant relationship between Theory of Mind commands and intelligence quotient ability (Figure 2).

Figure 2: IQ range scores in both countries (Iran and Sweden).
Discussion and Conclusion
The results of the present study show that children with a higher intelligence quotient perform better on ToM tasks in all cases reviewed, except for Smart_ RQ and SAR, which are not significant but follow the expected pattern.
To bridge the gap between ToM and higher IQ scores in various disorders, previous studies have documented a positive relationship between cognitive ability, verbal IQ, verbal mental age and first-order attributional performance [11,23-25]. For example, Bíró and Russell had a review that children with ASD with higher verbal IQ had comparatively better performance on both executive functions (EF) and ToM tasks based on the use of inner speech to regulate executive control over actions than children with lower verbal IQ [25,26].
Accordingly, the predictions for passing the ToM task with higher IQ are due to false belief attributions. Research by Bauminger & Kasari [24]. has shed light on the current issue. According to this, 22 children with HFA passed the belief questions and scored significantly higher than 19 typical peers on the Full and Verbal IQ tasks.
In solving specific features of the EF tasks, the low functioning autistic children (IQ range below 70) showed a delay in ToM development compared to the high functioning children (IQ score above 70). It is worth noting that in terms of false belief ability, the LFA group never arrived at false belief attributions [27].
The results of the current study provide further evidence of the importance of cognitive ability in children with ASD and DS for performance on false belief tasks and intelligence quotient. It adds to the existing literature on underreporting of false beliefs with a higher intelligence quotient in the autism, Down syndrome and typically developing groups of children. Children with higher intelligence quotients perform better on ToM tasks, regardless of the group to which they belong. As a particular potential ToM study, it is relevant to other clinical groups.
Limitations: An important limitation in the choice of instruments was the choice of tests translated into Farsi and Swedish, which limited the possibility of measuring ToM broadly in other ways. Therefore, future studies should explore other methods and instruments to examine false beliefs and ToM skills as well as intelligence quotient in the clinical groups.
Author Statements
Acknowledgements
We would like to thank all those who participated in this study.
References
- Abrahams BS, Geschwind DH. Advances in autism genetics: on the threshold of a new neurobiology. Nature reviews genetics. 2008; 9: 341-355.
- Carr J. Six weeks to twenty-one years old: a longitudinal study of children with Down’s syndrome and their families. Child Psychol Psychiatry Allied Disc. 1988; 29: 407–31.
- Baddeley A, Jarrold C. Working memory and Down syndrome. Journal of Intellectual Disability Research. 2007; 51: 925-931.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5®): American Psychiatric Pub. 2013.
- World Health Organization. The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. World Health Organization. 1992; 1.
- Deci EL, Ryan RM. Handbook of self-determination research: University Rochester Press. 2002.
- Anto Praveen R. Relationship between Theory of Mind and Intelligence among Children. Christian Medical College, Vellore. 2007.
- Kaland N, Møller-Nielsen A, Callesen K, Mortensen EL, Gottlieb D, Smith L. A new advanced test of theory of mind: evidence from children and adolescents with Asperger syndrome. Journal of child psychology and psychiatry. 2002; 43: 517-528.
- Sanz-Cervera P, Pastor-Cerezuela G, Fernández-Andrés MI, Tárraga-Mínguez R. Sensory processing in children with autism spectrum disorder: relationship with non-verbal IQ, autism severity and attention deficit/hyperactivity disorder symptomatology. Research in Developmental Disabilities. 2015; 45: 188-201.
- Buitelaar J, Van der Wees M, Swaab-Barneveld H, Van der Gaag R. Verbal Memory and Performance IQ Predict Theory of Mind and Emotion Recognition Ability in Children with Autistic Spectrum Disorders and in Psychiatric Control Children. The Journal of Child Psychology and Psychiatry and Allied Disciplines. 1999; 40: 869-881.
- Happé FG. Wechsler IQ profile and theory of mind in autism: A research note. Journal of Child Psychology and Psychiatry. 1994; 35: 1461-1471.
- Raven JC. Mental tests used in genetic studies: The performance of related individuals on tests mainly educative and mainly reproductive. Unpublished master’s thesis, University of London. 1936.
- Raven JC, Court JH, Raven J. Raven’s Colored Progressive Matrices. Dr. G. Schuhfried Ges M. B. H. Austria. 2002.
- Raven J, Raven JC, Court JH. Standard progressive matrices, 1998edition. Oxford, England: Oxford Psychological Press. 1998.
- Raven JC, Court JH, Raven J. Manual for Raven’s progressive matrices and vocabulary scales: American and international norms. Oxford, England: Oxford Psychological Press. 1990.
- Dahlgren S, Sandberg AD, Larsson M. Theory of mind in children with severe speech and physical impairments. Research in developmental disabilities. 2010; 31: 617-624.
- Rajabi GR. Standardization of the Raven’s Progressive Matrices test in school children in Ahwaz. Contemporary Psychology. 2008; 3: 23-32.
- Wimmer H, Perner J. Beliefs about beliefs: Representation and constraining function of wrong beliefs in young children’s understanding of deception. Cognition. 1983; 13: 103-128.
- Baron-Cohen S, Leslie AM, Frith U. Does the autistic child have a “theory of mind”?. Cognition. 1985; 21: 37-46.
- Perner J, Leekam SR, Wimmer H. Three-year-olds’ difficulty with false belief: The case for a conceptual deficit. British journal of developmental psychology. 1987; 5: 125-137.
- Muris P, Steerneman P, Meesters C, Merckelbach H, Horselenberg R, van den Hogen T, et al. The TOM test: A new instrument for assessing theory of mind in normal children and children with pervasive developmental disorders. Journal of Autism and Developmental Disorders. 1999; 29: 67-80.
- Gopnik A, Astington JW. Children’s understanding of representational change and its relation to the understanding of false belief and the appearance-reality distinction. Child development. 1988; 59: 26-37.
- Yirmiya N, Solomonica-Levi D, Shulman C, Pilowsky T. Theory of mind abilities in individuals with autism, Down syndrome, and mental retardation of unknown etiology: The role of age and intelligence. Journal of Child Psychology and Psychiatry. 1996; 37:1003-1014.
- Bauminger N, Kasari C. Brief report: Theory of mind in high-functioning children with autism. Journal of autism and developmental disorders. 1999; 29: 81-86.
- Pellicano E. Links between theory of mind and executive function in young children with autism: clues to developmental primacy. Developmental psychology. 2007; 43: 974-90.
- Bíró S, Russell J. The execution of arbitrary procedures by children with autism. Development and Psychopathology. 2001; 13: 97-110.
- Robberts M. Theory of mind development: A comparison of children with autism spectrum disorders and typically developing South African children. Unpublished honours thesis, University of Cape Town, South Africa. 2008.